


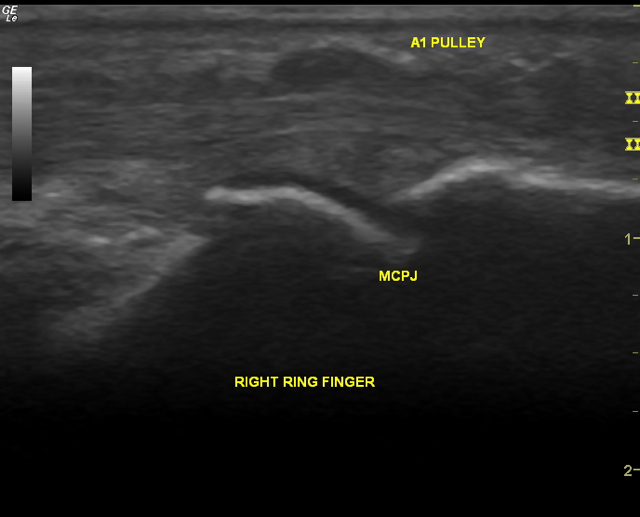
 Ultrasound (longitudinal view) of a trigger finger
Ultrasound (longitudinal view) of a trigger fingerLast weekend was spent with 31 rheumatology colleagues in a darkened room away from the beautiful Sydney sunshine.
We were learning ultrasound. Taught by Drs Fred Joshua, Anita Lee & Helen Keen. They are the leading the way for rheumatology ultrasound for us Aussies.
In Australia, ultrasound use by rheumatologists (in their own clinics as opposed to sending away a patient to some radiology service somewhere) is not widespread. At least, not yet. It's set to change.
I'd bought a portable ultrasound machine 4 years ago. It's a useful tool and has led to changes, and I believe, improvements in how I manage patients.
The weekend of discussion and the general enthusiasm among the group has invigorated my interest. I thought it worth sharing with you why I bother with using musculoskeletal ultrasound as a clinical rheumatologist:
- It's convenient. Both for the patient and the rheumatologist. Most rheumatologists using ultrasound will just have it handy in their clinic to use whenever it's required. It's relatively quick when targeted. There's no harmful radiation. And you may have your answer on the spot.
- It changes management. My more mature colleagues taught me that they were confident that they could feel synovitis with their fingers almost every time. I haven't found my fingers to be as sensitive as theirs. Sometimes, I need the ultrasound (or MRI) to help detect synovitis. Many rheumatic diseases can be difficult to diagnose. Sometimes, clinical signs are hard to find. Ultrasound can help with this.
- It improves compliance. I can't prove this but my feeling so far is that patients who see their pathology on the screen engage more with the disease as their understanding improves. An example is the patient with active rheumatoid arthritis who may be quite reluctant to have treatment. When that patient sees the damage occurring at their joints and/or the actual swollen tissues highlighted by the red-colour of aggressive blood vessels infiltrating the tissue, it makes it easier to progress a discussion about management.
- Patients like it. It's a bit of tech. Bits of the body can be moved dynamically and you can watch it happen on screen. It's easier to understand (still with lots of explanation) than the image slices of a MRI or CT.
- It helps guide difficult injections. I've used it to direct needles into specific parts of the body, such as the subacromial bursa of a shoulder with the patient able to follow the tip of the needle on screen into the correct space.
- It's interesting. It's nice to have a "toy" in rheumatology. I spend the day talking and listening, listening and talking. Unlike your high-powered, tool-using cardiologist or a scope-wielding gastroenterologist, rheumatologists don't/didn't have gadgets - until ultrasound.
As I write this, I actually think I've been underusing this tool. Time pressures are mostly to blame.
It will be great to have more rheumatology colleagues locally using musculoskeletal ultrasound in their daily practice. It has been very difficult to access training and I've found it difficult to improve my skills and knowledge due to the isolation and lack of support that comes with being one of a small handful of ultrasound-wielding rheumatologists in Australia.
Sharing knowledge, comparing images, being able to better calibrate what we each do can only lead to improved skill.
What is your experience with ultrasound in the hands of a rheumatologist? Did you find it useful?
